Este fondo ha logrado atraer a inversores como Sequoia Capital, y tiene previsto captar entre 180 y 270 millones de euros este mismo año. Posteriormente, la compañía cuenta con recaudar más de 900 millones de euros en un periodo de cuatro años.
El consejero delegado del grupo farmacéutico, Pascal Soriot, ha afirmado, en declaraciones recogidas por EFE, que AstraZeneca está construyendo un nuevo centro de investigación y un laboratorio de inteligencia artificial en la ciudad de Shanghái. En el mismo sentido, también ha asegurado que todas las multinacionales que conoce tienen su punto de mira en China.
...
13 noviembre 2019
Almirall . Los Gallardo venden el 6,3% de la Farmacéutica por 167,75 millones de euros. Los hermanos seguirán controlando casi el 60% de la farmacéutica . Post by Celtia .
REDACCIÓN | AGENCIAS, BARCELONA // 13/11/2019 .
 Los accionistas mayoritarios de la compañía farmacéutica Almirall, Antonio Gallardo y Jorge Gallardo, han vendido un 6,3% de la empresa por 167,7 millones de euros en una colocación acelerada que se anunció este martes por la tarde. Los Gallardo han informado esta mañana a la Comisión Nacional del Mercado de Valores (CNMV) del resultado de la colocación y han precisado que mantienen una participación del 59,7% en la empresa.
Los accionistas mayoritarios de la compañía farmacéutica Almirall, Antonio Gallardo y Jorge Gallardo, han vendido un 6,3% de la empresa por 167,7 millones de euros en una colocación acelerada que se anunció este martes por la tarde. Los Gallardo han informado esta mañana a la Comisión Nacional del Mercado de Valores (CNMV) del resultado de la colocación y han precisado que mantienen una participación del 59,7% en la empresa.
La venta, que equivale a 11 millones de títulos de la farmacéutica, se ha cerrado entre “inversores cualificados e institucionales” y con descuento de un 10%, ya que las acciones de Almirall cerraron este martes a 16,98 euros y el precio de venta unitario de esta colocación ha sido de 15,25 euros. Las acciones de la empresa retrocedían este miércoles en bolsa hasta ese precio, con una caída del 10%.
...

La venta, que equivale a 11 millones de títulos de la farmacéutica, se ha cerrado entre “inversores cualificados e institucionales” y con descuento de un 10%, ya que las acciones de Almirall cerraron este martes a 16,98 euros y el precio de venta unitario de esta colocación ha sido de 15,25 euros. Las acciones de la empresa retrocedían este miércoles en bolsa hasta ese precio, con una caída del 10%.
...
ZEPSYRE® Clinical Trial is Showing Promising Results for Mesothelioma Patients .
2 Links :
*.- Zepsyre® en Monoterapia es Activo en Mesothelioma Pleural Maligno .
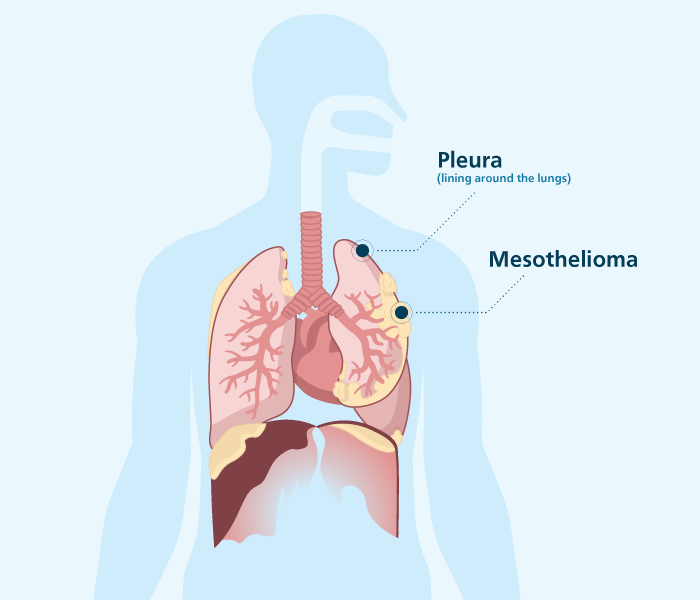
*.- What Is Pleural Mesothelioma?.
 Pleural mesothelioma is a rare malignant cancer. Almost 75% of diagnosed mesothelioma cases form in the pleura, making it the most common of the four types.
Pleural mesothelioma is a rare malignant cancer. Almost 75% of diagnosed mesothelioma cases form in the pleura, making it the most common of the four types.
*.- Zepsyre® en Monoterapia es Activo en Mesothelioma Pleural Maligno .
*.- What Is Pleural Mesothelioma?.

The cause of pleural mesothelioma is exposure to asbestos fibers, which are inhaled into the lungs. It usually takes from 20 to 50 years for mesothelioma to develop after a person’s first exposure to asbestos. Because of this latency period, the disease usually affects people older than 75.
The average life expectancy for pleural mesothelioma is often less than 18 months, but it depends on many factors.
Although there is no cure for mesothelioma, some patients live much longer with treatments. Combining several treatments, such as surgery, chemotherapy and radiation therapy, has helped some people live for years. Clinical trials offer access to new treatments such as immunotherapy.
Pleural Mesothelioma Facts
- Most common type of mesothelioma
- Forms on soft tissue covering the lungs
- Symptoms: Shortness of breath, chest pain, dry cough and fatigue
- Diagnostic Tools: Imaging scans and tissue biopsies
- Treatments: Chemotherapy, surgery, radiation therapy, immunotherapy and experimental therapies
- Life Expectancy: About 40 percent live at least one year
...
Zepsyre® . Para el Tratamiento de Cáncer de Pulmón Microcítico . Más Opiniones Favorables de Oncólogos .

Dr . Taofeek K. Owonikoko, MD, PhD :

Por lo que Zepsyre® es particularmente efectivo en Pacientes con Enfermedad Quimio-Sensible. Y el mecanismo de acción también es racional para la Enfermedad Pulmonar de células Pequeñas, que ahora sabemos que es un Tumor Adicto a la Transcripción. Este es un Agente que Funciona Inhibiendo la Función de la ARN Polimerasa y, por lo tanto, evitando que ocurra la Transcripción.
Esperamos que podamos contar pronto con el Farmaco ya para uso Clinico a traves de una Aprobación Regulatoria para ello .
***********************************
DLL3-Targeted and Chemo-Sensitive Therapy .
Panelists: Naiyer A. Rizvi, MD, NewYork-Presbyterian Hospital; Taofeek K. Owonikoko, MD, PhD, Winship Cancer Institute of Emory University ; Ticiana Leal, MD, University of Wisconsin-Madison; Jamie E. Chaft, MD, Memorial Sloan Kettering Cancer Center .
Published: Monday, Nov 11, 2019 .
Naiyer A. Rizvi, MD:
We are waiting for a lot of the additional immunotherapy data, such as the DURVA [durvalumab]–TREME [tremelimumab] arm of the CASPIAN trial, to read out. But I think we have options first-line. We discussed second-line options. And we really want to just kind of look at the literature and see what’s next. I’ll pick on Jamie because she was involved in this trial—not directly, but she treated some of the patients on the DLL3-targeting therapy with Rova-T [rovalpituzumab tesirine]. Do you want to talk about your experience with this and why it’s so difficult to develop drugs in small cell lung cancer?
Jamie E. Chaft, MD:
DLL3 was a hugely exciting target and still is. There are multiple new drugs in development targeting DLL3 as a part of the notch signaling pathway. Developmentally it makes sense to target. And I think we saw an expression-based response. So immunohistochemistry for DLL3, enriched to response to the agent, Rova-T [rovalpituzumab tesirine]. We were just limited by toxicity.
The drug, while effective, was exceptionally hard on patients, including severe life-threatening toxicities, notably edema and infusions. To my understanding the development of the initial DLL3...is done. But I think we’re still enthusiastic about DLL3 as a target. It’s expressed particularly in certain subsets of small cell and up to two-thirds. And this should be a promising target for the future within other immune-directed approaches by specific antibodies, CAR-T cells [cancer antigen receptor T cells], things like that.
Naiyer A. Rizvi, MD:
Taofeek, I know you’ve been involved in the lurbinectedin experience. When I look at the data it’s pretty impressive, and you’ve been very involved in these trials. I’d love to hear more about this agent and where you see its future.

Taofeek K. Owonikoko, MD, PhD:
In the interest of full disclosure, I’ve actually not been directly involved with the trial, but I’ve been following the data, and some of the investigators there, like the rest of us, we’re good friends. So I think the lurbinectedin is a very interesting compound. At least based on what we now know from published data presented at meetings, this is an agent that seems to be particularly effective in patients with chemo-sensitive disease. And the mechanism of action also is rational for small cell lung disease, which we now know to be a transcriptionally addicted tumor. This is an agent that works by inhibiting RNA polymerase to function, and therefore preventing transcription to occur.
The earliest evidence that this could be an agent that we’d use in our patient population came from the doublet trial looking at the combination of lurbinectedin with doxorubicin. And that was from the attempt originally to develop this in sarcoma patients where doxorubicin was the backbone. They just layered this on. And they saw some signal then that led to the launching of the ATLANTIS trial, which is the randomized phase III trial of that combination versus standard of care.
In retrospect, the observation was then made that perhaps for this group of patients, maybe you don’t need a doublet. They went back to now do the single-agent trial, which is now what is looking really promising and was not that different from what they saw with the original single-arm phase II trial with the doublet chemotherapy. We did the overall response rate about 35%. But when you look at patient with chemotherapy-sensitive disease, that’s actually close to 50%. For those with chemotherapy-resistant disease it’s low double digits, maybe around 20%. But regardless of whether you’re chemotherapy sensitive or refractory, or chemotherapy resistant, there is something to be said for this agent in relapsed small cell.
The disappointment I see with this is that despite the higher response rates, you know, PFS [progression-free survival] was still around 5 months. Overall survival around 9 months. I think for the [chemo-therapy] sensitive, perhaps up to about 12 months, which is still better than what we have now. Whether this will become standard of care that we can use for our patient outside the ongoing clinical trials remains to be seen. We will know maybe a little later this year or early next year whether there will be regulatory approval for it. That is where we stand with this agent.
Transcript Edited for Clarity.
Suscribirse a:
Entradas (Atom)